-
Americas

-
Asia & Oceania

-
A-I
J-Z

EMEA Thought Leadership
Developing IQVIA’s positions on key trends in the pharma and life sciences industries, with a focus on EMEA.
Learn more -
Middle East & Africa

EMEA Thought Leadership
Developing IQVIA’s positions on key trends in the pharma and life sciences industries, with a focus on EMEA.
Learn more
Regions
-
Americas
-
Asia & Oceania
-
Europe
-
Middle East & Africa
-
Americas
-
Asia & Oceania
-

Europe
Europe
- Adriatic
- Belgium
- Bulgaria
- Czech Republic
- Deutschland
- España
- France
- Greece
- Hungary
- Ireland
- Israel
- Italia
EMEA Thought Leadership
Developing IQVIA’s positions on key trends in the pharma and life sciences industries, with a focus on EMEA.
Learn more -
Middle East & Africa
EMEA Thought Leadership
Developing IQVIA’s positions on key trends in the pharma and life sciences industries, with a focus on EMEA.
Learn more
SOLUTIONS
-
Research & Development
-
Real World Evidence
-
Commercialization
-
Safety & Regulatory Compliance
-
Technologies
LIFE SCIENCE SEGMENTS
HEALTHCARE SEGMENTS
- Information Partner Services
- Financial Institutions
- Global Public Health
- Government
- Patient Associations
- Payers
- Providers
THERAPEUTIC AREAS
- Cardiovascular
- Cell and Gene Therapy
- Central Nervous System
- GI & Hepatology
- Infectious Diseases and Vaccines
- Oncology
- Pediatrics
- Rare Diseases
- View All

Impacting People's Lives
"We strive to help improve outcomes and create a healthier, more sustainable world for people everywhere.
LEARN MORE
Harness the power to transform clinical development
Reimagine clinical development by intelligently connecting data, technology, and analytics to optimize your trials. The result? Faster decision making and reduced risk so you can deliver life-changing therapies faster.
Research & Development OverviewResearch & Development Quick Links

Real World Evidence. Real Confidence. Real Results.
Generate and disseminate evidence that answers crucial clinical, regulatory and commercial questions, enabling you to drive smarter decisions and meet your stakeholder needs with confidence.
REAL WORLD EVIDENCE OVERVIEWReal World Evidence Quick Links

See markets more clearly. Opportunities more often.
Elevate commercial models with precision and speed using AI-driven analytics and technology that illuminate hidden insights in data.
COMMERCIALIZATION OVERVIEWCommercialization Quick Links

Service driven. Tech-enabled. Integrated compliance.
Orchestrate your success across the complete compliance lifecycle with best-in-class services and solutions for safety, regulatory, quality and medical information.
COMPLIANCE OVERVIEWSafety & Regulatory Compliance Quick Links

Intelligence that transforms life sciences end-to-end.
When your destination is a healthier world, making intelligent connections between data, technology, and services is your roadmap.
TECHNOLOGIES OVERVIEWTechnology Quick Links
CLINICAL PRODUCTS
COMMERCIAL PRODUCTS
COMPLIANCE, SAFETY, REG PRODUCTS

BLOGS, WHITE PAPERS & CASE STUDIES
Explore our library of insights, thought leadership, and the latest topics & trends in healthcare.
DISCOVER INSIGHTSTHE IQVIA INSTITUTE
An in-depth exploration of the global healthcare ecosystem with timely research, insightful analysis, and scientific expertise.
SEE LATEST REPORTS



FEATURED INNOVATIONS
-
IQVIA Connected Intelligence™
-
IQVIA Healthcare-grade AI™
-
Human Data Science Cloud
-
IQVIA Innovation Hub
-
Decentralized Trials
-
Patient Experience Solutions with Apple devices
WHO WE ARE
- Our Story
- Our Impact
- Commitment to Public Health
- Code of Conduct
- Environmental Social Governance
- Privacy
- Executive Team
NEWS & RESOURCES


Unlock your potential to drive healthcare forward
By making intelligent connections between your needs, our capabilities, and the healthcare ecosystem, we can help you be more agile, accelerate results, and improve patient outcomes.
LEARN MORE
IQVIA AI is Healthcare-grade AI
Building on a rich history of developing AI for healthcare, IQVIA AI connects the right data, technology, and expertise to address the unique needs of healthcare. It's what we call Healthcare-grade AI.
LEARN MORE
Your healthcare data deserves more than just a cloud.
The IQVIA Human Data Science Cloud is our unique capability designed to enable healthcare-grade analytics, tools, and data management solutions to deliver fit-for-purpose global data at scale.
LEARN MORE
Innovations make an impact when bold ideas meet powerful partnerships
The IQVIA Innovation Hub connects start-ups with the extensive IQVIA network of assets, resources, clients, and partners. Together, we can help lead the future of healthcare with the extensive IQVIA network of assets, resources, clients, and partners.
LEARN MORE
Proven, faster DCT solutions
IQVIA Decentralized Trials deliver purpose-built clinical services and technologies that engage the right patients wherever they are. Our hybrid and fully virtual solutions have been used more than any others.
LEARN MORE
IQVIA Patient Experience Solutions with Apple devices
Empowering patients to personalize their healthcare and connecting them to caregivers has the potential to change the care delivery paradigm.
LEARN MOREWORKING AT IQVIA
Our mission is to accelerate innovation for a healthier world. Together, we can solve customer challenges and improve patient lives.
LEARN MORELIFE AT IQVIA
Careers, culture and everything in between. Find out what’s going on right here, right now.
LEARN MORE
WE’RE HIRING
"Improving human health requires brave thinkers who are willing to explore new ideas and build on successes. Unleash your potential with us.
SEARCH JOBSBlog
The Impact of COVID-19 on Cancer Treatment Across the EU4 + UK Countries
Jul 29, 2020
DOWNLOAD THE COUNTRY REPORTS HERE:
EU4 + UK | UK | ITALY | FRANCE | SPAIN | GERMANY | JAPAN | US
On March 10th 2020, the WHO declared COVID-19 was a pandemic. Three days later it announced that Europe had become the epicenter of the pandemic. Countries across Europe began taking measures to contain the spread of the virus in different ways.

We can all agree that these are unprecedented and challenging times for the entire healthcare industry. But looking deeper, at the unique effects the pandemic is having on certain sectors, stakeholders, and therapy areas, is valuable. Here we discuss the impact on the oncologist community, not just across the EU5 countries but across the globe, and the extent to which they have had to re-organize oncological care in a matter of weeks.
Cancer patients are amongst the most vulnerable populations, with or without COVID-19, and early, proactive detection has been a hallmark of treatment paradigms for the past few decades. Furthermore, oncology medicines and innovations are a significant market driver. And so, with lockdown measures restricting the movement and likely identification of patients, and healthcare systems being overwhelmed, we felt it critical to gather feedback from oncology specialists to understand from them directly what impact the pandemic is having on the treatment of cancer. Specifically, we wanted to dig deeper and to understand:
- The impact on cancer patient visits at different phases of the COVID -19 crisis: are oncologists seeing fewer cancer patients now compared to pre-COVID-19?
- The number of remote consultations conducted during different phases of the pandemic
- The specific types of cancer treatment practices are being impacted as a result of COVID-19
- The current changes anticipated to treatment practices now that restrictions are being relaxed in some areas of the world
- Initiatives Pharma companies can provide oncology specialists to help them deliver the best care possible to their patients, now and in the “new normal”
- The communication channels pharma companies are using to communicate with oncology specialists:
- During the lockdown
- Post-lockdown
- And what, in the view of oncology specialists themselves, this pattern could be 1-2 years down the line assuming COVID-19 no longer exists
Methodology:
Firstly, a very short 3-minute survey issued was hosted on our IQVIA’s internal and secure online community of healthcare professionals (HCPs) called DOCNET. Given the environment, and with a desire to avoid any unnecessary pressure on HCPs, IQVIA was very careful to not send reminders asking HCPs to complete the survey. The oncology specialists that completed the surveys did this voluntarily and no payment was made to them.
Secondly, to help us understand the impact of COVID-19 on the treatment of cancer, IQVIA gathered HCP feedback in April (Wave 1: April 2 – 8) during the height of the outbreak in Europe and when most countries were in lockdown. We also gathered feedback in June (Wave 2: June 17 – 22) after countries have started loosening restrictions.
IQIVA launched two waves in order to gauge the impact on cancer treatment during the lockdown and determine whether there were any changes in treatment of cancer post-lockdown.
Finally, this was a pulse survey. Questions were intended to provide top-level insights into the impact of COVID-19 on cancer treatment; this is not an exhaustive quantitative study. It’s also important to note that sample sizes were relatively small and might not be representative at country level. Sample sizes are also varied between the survey conducted in April and the one in June. When making cross country comparisons, please also be aware that sample composition are different between countries.
Improvement in patients visits rate, however number of patient visiting is below pre-COVID -19
There has been an overall improvement in patient visit rates due to the easing of restrictions across the EU5 countries. In April, oncology specialists were seeing 52% fewer patients per week. In June and after ease of restriction they now seeing 36% fewer patients. For example, at the UK country level, improvements in the number of patients seen per week is noticeably better in June vs April where oncology specialists see 38% fewer patients per week vs 66% per week in April – an improvement of a 28-percentage points.
While there is an overall improvement in patients visits rate in June compared to April, the actual number of patients is still relatively low compared to pre-COVID-19.
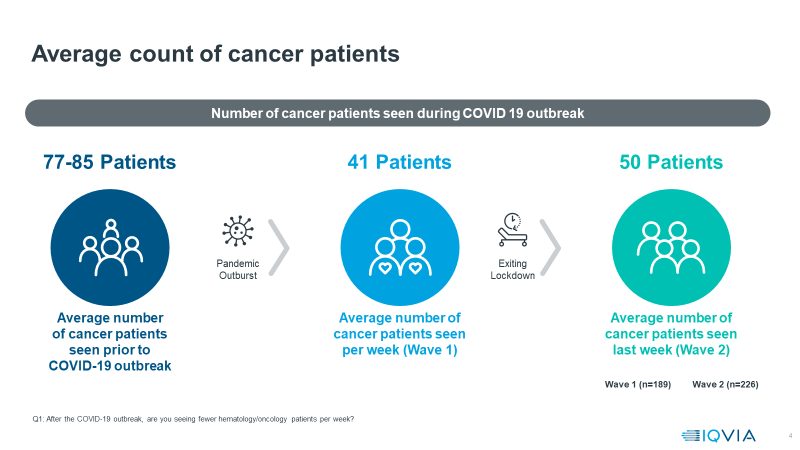
On average, oncology specialists were seeing 81 patients per week pre COVID-19. That number decreased significantly, to 41 patients in April (Wave 1) at the start of the pandemic and during lockdown.
Post lockdown, we are seeing that number increase to 50 patients per week, but this is still far less than the average seen prior to the outbreak. So, we can be optimistic in the trend, and see signs of hope that treatment practices have started, albeit slowly, to return to some level of normality.
As always, it is worth looking at the outliers as it gives us a sense of heterogeneity in the experience of COVID-19 around the world. Our general insights above notwithstanding patient visits are currently higher in Germany than they are in other markets. Here, hem-oncologists pre-COVID-19 were seeing an average of 141 patients per week, and that number decreased to 75 in April (Wave 1) during lockdown; now in June (Wave 2) and post-ease of restrictions, the average number of patients seen has risen to 112. In France, the average number of patients seen has not increased post-ease of restriction.
Increase in remote consultation done by telehealth as a result of COVID-19
The mode of interaction between oncology specialists and cancer patients has changed as a result of COVID-19. It’s important to note that this trend is also seen across the board by all healthcare professionals; it’s not unique to oncology specialists.
During the lockdown period (as illustrated by the chart below), we see that there was a significant increase in remote patient consultations done by telehealth at a total EU5 level. When asked what percentage of their consultations were done remotely prior to the COVID-19 pandemic, oncology specialists across the EU5 said that only 6% of consultations were done remotely. We now see that percentage has increased significantly to 56% during the lockdown period.
In June, and as countries start existing lockdown, we note that the percentage of remote consultations is still relatively high (as compared to the admittedly low baseline), at 34%. Interestingly, when asked about what will happen when COVID-19 ceases to exist, physician believe that nearly 20% of their consultation moving forward will continue to be done remotely.
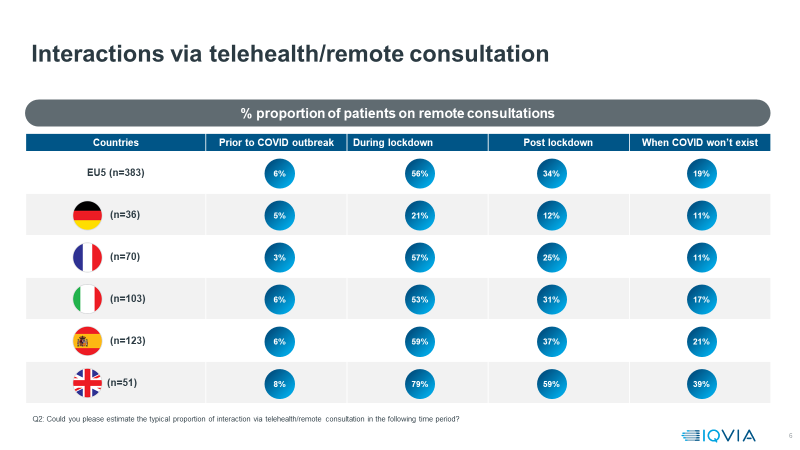
This is particularly true for the UK where oncology specialists see more remote consultations becoming part of their practice to a higher extent than other countries.
There has been an impact on cancer treatment practices as a result of COVID-19
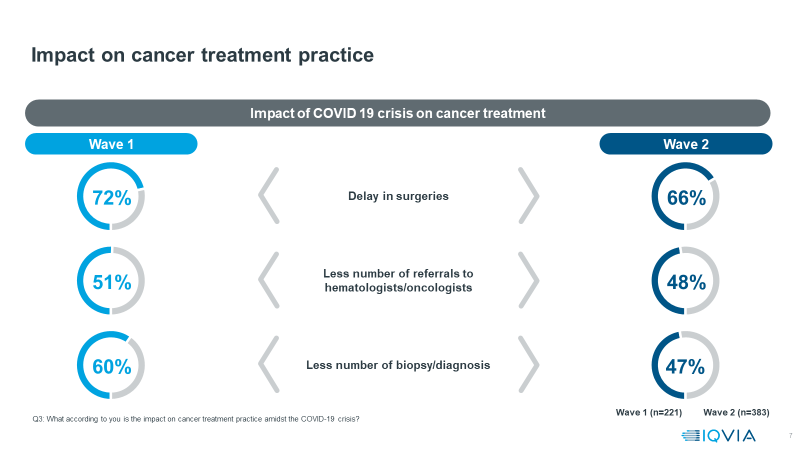
Delays in surgeries, delays in chemo and a reduction in the number of biopsies are the top 3 practices in the treatment of cancer that have been most impacted as a result of the COVID-19 pandemic. This was true in April during the height of the pandemic and continues to hold true in June as countries have started easing movement restrictions.
As countries begun ease of movement restrictions the reduction in biopsies and diagnoses being conducted is reduced to 47%, compared to 60% in April (Wave 1).
Similarly, delays in surgeries have also dropped to 66% from 72% during the June lockdown period (Wave 2).
To better understand what key changes oncology specialists are currently experiencing in their practice setting, we grouped responses into 3 categories: changes that will impact Patients, changes that will impact oncology specialists and changes seen in Hospital settings.
-
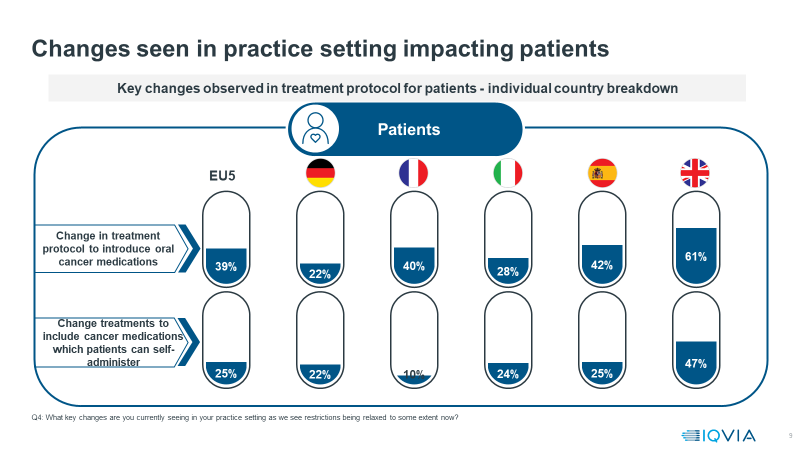
Treatment practice changes impacting Patients:
- Nearly 40% of oncology specialists said that they will now introduce oral cancer medications to patients
- 1 in 5 specialists said that they would include cancer medications which patients can self-administer
- In the UK, 60% of oncology specialists are currently introducing more oral medications whilst nearly 5 in 10 are introducing cancer medications which patients can self-administer. In Spain and France, nearly 40% are introducing more oral medications.
- Treatment changes impacting oncology specialists:
- Switching to remote consultation is the biggest change anticipated
- Nearly 3 in 10 specialists said they will have to increase their daily working hours, work over the weekend to conduct more chemotherapy cycles and conduct surgeries to compensate for backlogs caused as a result of the lockdown
- Changes impacting Hospital settings:
- Nearly 60% said that its limiting visitor policy except in case of end of life circumstances
E-mails, webinars and virtual meetings are now dominant communication channels
It’s not surprising that when we asked oncology specialists how Pharma companies are communicating with them now, the vast majority said that e-mails, webinars and virtual meetings have become the dominant communication channels - a sentiment supported by broader research, including IQVIA’s ChannelDynamicsTM .
ChannelDynamicsTM data suggests that countries that were more reliant on face-to-face (F2F) interactions, such as the UK and France, witnessed a decline in overall interaction volumes. On the other hand, Germany, which already relied upon remote engagement tools, saw an increase in overall interactions. It’s important to note that ChannelDynamicsTM data is not oncology specific.
There is, of course, a natural backlog that is building from the reduction in visits, patient interactions, biopsies, etc. Oncology specialists are looking to Pharma companies to help them manage the anticipated surge in cancer patients in the coming months by increasing patient support services, providing updates on the availability of critical oncology drugs for their patients, sharing tips on how to best communicate remotely with the rest of their practice and patients, and make available online resource centers which can be accessed for product-related information.
What are the potential implications of for Pharma Companies?
Now more than ever, pharma companies are looking for ways to improve patient care and outcomes. How they support physicians going forward -particularly in oncology -will make a big difference. To that end, below are some thoughts on actions that can be taken by Pharma companies.
- Patient backlog created by reduced patient visits during the lockdown
- It will be critical that Pharma companies support oncology specialists by helping them understand how to manage workload associated with increased patient backlog, less time to spend with patients, and less time to engage with pharma companies.
- Delays in diagnosis, treatment starts, treatment switching and treatment decisions
- It will be vital for pharma companies to research and quantify the impact of patient backlog on patient treatment and brand use. This can feed into forecast revisions and identification of improved paths to treatment, including support for home/self-treatment
- Changes to Oncology specialist’s interaction and treatment
- Pharma companies must keenly understand how patient interactions are changing and determine the types of support that can be made available to oncology specialists. Pharma companies will need to research and act on changed physician engagement preferences
The impact of this pandemic on the Oncology market will provide learnings to pharmaceutical companies across other therapy areas both in the short and the long term. Oncology is pharma’s single most valuable pharmaceutical market and will continue to be the world’s most valuable market, driven by more innovation throughout the next decade and beyond. However, the COVID-19 pandemic crisis has clearly had considerable impact on the practice of cancer treatment, the consequences of which will be felt for some time to come.
Cancer remains the second leading cause of death in European nations. As such, it is of huge public health concern, and in cancer treatment, early diagnosis and rapid treatment with the right modalities remain the most effective route to reduce mortality and improve survival. If healthcare systems struggle, in the post pandemic crisis world, to bring cancer treatment back to its previous efficiency, the consequences for some patients could be serious. Pharmaceutical companies, for which cancer represents the most valuable, and the most innovative, sector of their prescription medicine market, must play an active part in addressing this. This will require them first, to understand in greater detail where the roadblocks to effective treatments are, for patients and healthcare professionals, and then how investments and actions they as companies can take which would help address those, and ensure that cancer treatment not only regains its prior effectiveness in terms of speed and availability of treatments, but comes back more customer-centric and effective than before, due to the adoption of new technologies and approaches.